
For a couple of years now, The U.S. Preventive Services Task Force (a group of experts that makes recommendations to the U.S. Department of Health and Human Services) has been trying to change accepted medical guidelines on screening mammography for women. It should be noted that prior guidelines recommended screening for breast cancer start at age 40 and continue for as long as the woman is in good health. The new government recommendations now state that screening not start until age 50, be performed every other year rather than every year, and cease when a woman reaches age 75. There are guidelines for woman with a higher than normal risk of breast cancer and for those who feel a lump. However, the new guidlines, found here: http://www.uspreventiveservicestaskforce.org/Page/Document/UpdateSummaryFinal/breast-cancer-screening are not wholeheartedly supported by most in the medical community.
 The American Cancer Society has altered it’s previous views on mammography screening to jive just a little bit better with the government’s recommendations, by changing the initial age to begin screening from age 40 to age 44-45, but they still recommend yearly mammograms vs. every other year, and they do NOT discourage mammograms before age 50 as the media tried to allude to earlier this week.
The American Cancer Society has altered it’s previous views on mammography screening to jive just a little bit better with the government’s recommendations, by changing the initial age to begin screening from age 40 to age 44-45, but they still recommend yearly mammograms vs. every other year, and they do NOT discourage mammograms before age 50 as the media tried to allude to earlier this week.
It should also be noted that the conclusions made by The US Preventive Task Force are based on the public health perspectives of the effect of breast cancer screening. It looks at how women who have negative biopsies are traumatized by the fear of a possible breast cancer diagnosis and the cost to public health when a biopsy is “unnecessary.” It doesn’t explain that the biopsy was NOT unnecessary. There was an abnormal area on a mammogram AND another imaging modality, either ultra sound and/or breast MRI and that abnormality could not be listed as benign without further testing. That further testing came in the form of a biopsy, which BTW, is the only true way to test for breast cancer. So, the fact remains there was an abnormality in the breast that needed to be removed and the patient was damned lucky it was NOT cancer. That, in my opinion, is a blessing and not an unnecessary test.
Secondly, the researchers were looking at how changing breast cancer screening guidelines affect the overall public, rather than the individual. Researchers looked at tens of thousands of medical records of patients who were screened, diagnosed, and subsequently treated for breast cancer. They used a computer model taking into account certain medical data and assumptions about breast cancer diagnosis and treatments to determine the benefits and risks of changing breast cancer screening guidelines. They concluded that breast cancer was less prevalent in women under 50 and therefore, women under 50 didn’t need routine screening if there was no family history or other risk factors for breast cancer.
What they did NOT take into account was the fact that breast cancer is more common in women over 75, so why discourage breast cancer screening after age 74? They also failed to take into account that in women under 50, breast cancer is much more aggressive. It tends to grow faster and metastasize faster. It means  that without early detection, breast cancer in women under 50 is not only less treatable, resulting in more aggressive treatment protocols such as mastectomies vs, lumpectomies, it is less curable, resulting in a higher mortality rate.
that without early detection, breast cancer in women under 50 is not only less treatable, resulting in more aggressive treatment protocols such as mastectomies vs, lumpectomies, it is less curable, resulting in a higher mortality rate.
Another fact to consider is that by the time a woman has a palpable lump which proves to be breast cancer, the disease is already active and growing, which usually means a higher stage of the disease. Why wait until you have a lump in your breast if you can have a screening mammogram each year after age 40 to prevent that lump from growing and spreading?
The new guidelines do make allowances for women with a higher risk of breast cancer. Those risk factors include:
*Family history of breast cancer ( mostly in first degree relatives: mother, maternal grandmother, maternal aunt, sister, daughter)
*Personal history of benign biopsies.
*Does the woman carry the BRCA 1 or BRCA2 gene?
*Woman’s age (over 50)
*Woman’s age at first menstrual cycle- under age 13=higher risk factor for breast cancer
*Childbirth- not having children increases a woman’s risk of breast cancer
*Age when first childbirth occurred- women who postpone childbirth until after age 30 are at higher risk for breast cancer.
*Breast feeding- not breast feeding increases a woman’s risk of breast cancer
*Palpable lumps and or masses in breasts
* Use of birth control pills
If you’d like to take your own breast cancer assessment test, you can find it online at http://www.cancer.gov/bcrisktool/

 I was 47 when I was diagnosed with breast cancer after a routine screening mammogram. I had no symptoms, I had no family history, and I only met one of the risk factors for breast cancer. I took birth control pills.
I was 47 when I was diagnosed with breast cancer after a routine screening mammogram. I had no symptoms, I had no family history, and I only met one of the risk factors for breast cancer. I took birth control pills.
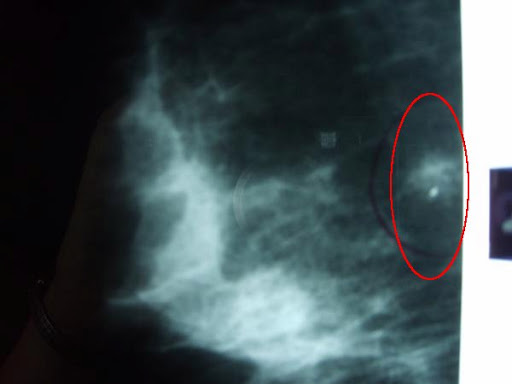
My cancer was aggressive as cancers tend to be in women under 50, and it was close to the chest wall. It had a high proliferation rate, which meant it was increasing and spreading at a rapid pace.

Biopsy specimen
The lesion was already between the sizes it should be for stage one diagnosis, but because of screening mammography, the doctors caught it before it reached stage two. Had I waited until I felt a palpable lump or until I was 50, I most likely would not be here now.
As a mammographer, far too often, I see women who postponed their screening mammogram until they felt a lump or turned 50, only to learn they have a more advanced stage of breast cancer that could have been caught sooner had they begun screening at age 40.
The U.S. Preventive Services Task Force did use researchers and doctors to come up with these new guidelines, but they were family doctors, scientific researchers and OB/Gyn’s. They were not radiologists, radiation oncologists, or medical oncologists. They were not doctors who deal with breast cancer on a routine basis.
Another fact: Neither the Breast Cancer Organization, the FDA, nor the American College of Radiology agree with The U.S. Preventive Services Task Force’s findings.
The FDA, also a government agency, is the governing body that oversees MQSA (Mammography Quality Standards Act.) They ensure compliance with radiation safety, quality control, the credentials, registration, and continuing education of all technologists who perform mammograms, the radiologists who interpret the mammograms, and the physicists who ensure the accuracy of all mammography equipment, and the FDA still recommends annual screenings begin at age forty.
The FDA has other guidelines that all certified sites must follow. Facilties that perform mammograms must send out letters to the patient directly as well as full reports to the ordering physician. These letters must inform the patient if their mammogram results are normal or if they need to follow up with their physician. If the letter advises them to follow up, it means additional imaging is recommended in the form of a diagnostic mammogram, ultrasound, short term follow up, and/or biopsy. The FDA also requires the letters to give information on a patient’s breast density. The site where I perform mammograms recommends the site http://www.areyoudense.org/
If this is not enough information to help you decide whether to screen at 40 vs. 50, here are some other facts to consider.
Currently, the government requires Medicare Part B and Medicaid to cover screening mammograms without a copay or deductible on women over 40 if the doctor or other qualified health care provider accepts assignment. Raising the screening age to 50 will save the government money. Insurance companies normally fall in line with medicare/medicaid guidelines, which means most insurance companies would no longer pay for screening mammograms for patients with medium to no risk risk factors for women under 40 if medicare raises the age. Patients will then either not have the study done, or they will pay out of pocket as they were forced to do back in the 80’s.
Insurance companies and the government will save money and the cure rate for breast cancer will rise to the level it was back in the late 80’s and early 90’s before insurance companies began covering screening mammograms. Or, doctors will start ordering more diagnostic mammograms so their patients will get the health studies they need by claiming breast pain or lumps, both of which are payable reasons for a diagnostic mammogram and neither of which can be disproved since breast tissue is naturally lumpy. Since diagnostic mammograms take 2 to 3 times longer to perform than screening mammograms because of additional images and the need to show the radiologist the films, this will result in scheduling delays and longer wait times because of a surge in the need for diagnostic imaging. It will also result in an increase in cost because diagnostic mammograms cost more than screening mammograms and in an increase in radiation exposure to the patient because more images are acquired during a diagnostic vs. a screening study.
As far as the Task “Force claiming screening women younger than age 50 leads to an increase in the number of normal or benign biopsies, the FDA has had guidelines in place for years to deal with this issue. All certified facilities who perform mammograms must also perform annual audit trails. These facilities track the number of biopsies ordered and performed by each and every radiologist who interprets mammograms and the number of those biopsies that are positive. The goal is for the positive rate to be at 25% or higher, which lets the radiologist and the FDA know if too many biopsies are being ordered. The good news for women is that of all biopsies performed, only about 1/4 are positive for breast cancer. That doesn’t mean the biopsy was unnecessary. As stated before, there are other abnormal findings in the breast that are not cancer, but still need addressing, such as atypical hyperplasia, fibroadenomas, and some infectious processes.
 Now as always, the best defense against breast cancer is early detection. And according to the ACR Appropriateness Criteria:
Now as always, the best defense against breast cancer is early detection. And according to the ACR Appropriateness Criteria:
Mammography is the only method of screening for breast cancer shown to decrease mortality.
 1 in 8 women (some studies say 1-7 women thanks to early detection) will develop breast cancer in her lifetime.
1 in 8 women (some studies say 1-7 women thanks to early detection) will develop breast cancer in her lifetime.
 mammograms in the form of digital and more recently, 3D mammograms, and screening programs put into place that not only recommend screening at age 40, but programs like Komen for the Cure and local health departments that assist low income and uninsured women get the screening studies they need. If the government succeeds in raising the screening age to 50 nationwide and all insurance companies, medicaid, and medicare comply, the government and insurance companies will benefit by saving money and/or increasing profits, but there will be a rise in the mortality rate of breast cancer.
mammograms in the form of digital and more recently, 3D mammograms, and screening programs put into place that not only recommend screening at age 40, but programs like Komen for the Cure and local health departments that assist low income and uninsured women get the screening studies they need. If the government succeeds in raising the screening age to 50 nationwide and all insurance companies, medicaid, and medicare comply, the government and insurance companies will benefit by saving money and/or increasing profits, but there will be a rise in the mortality rate of breast cancer.
